Although federal officials are touting the benefits of electronic health records, many health care providers and experts are worried that EHRs will not deliver on their promise, the Pittsburgh Post-Gazette reports.
In 2009, federal lawmakers passed the HITECH Act as part of the federal economic stimulus package. The act allows health care providers who demonstrate meaningful use of certified EHRs to qualify for incentive payments through Medicare and Medicaid.
Concerns About EHR Implementation
However, many physicians, particularly those in small practices, are expressing concern about the cost and time involved with implementing EHR systems.
Jaan Sidorov, a health care consultant, said, “The thing about these systems is that it doesn’t really look like they’re getting any cheaper. And the upgrades and the upkeep represent a very significant cost, especially in outpatient clinics.”
Some experts also have expressed concern that there have been few rigorous studies to prove that EHRs reduce health care costs or improve patient outcomes. A Public Library of Science study by doctors in the United Kingdom noted that “there is a large gap between the postulated and empirically demonstrated benefits of e-health technologies (and) their cost-effectiveness has yet to be demonstrated, despite being frequently promoted by policymakers and ‘techno-enthusiasts.'”
Ken Adler, medical director of IT at Arizona Community Physicians, said, “There is no really good data that shows that [EHRs] reduce hospitalizations. The nation is investing a huge amount of money on a hope and prayer” (Toland, Pittsburgh Post-Gazette, 8/7).
Source: iHealthBeat
This week, Reps. Karen Bass (D-Calif.) and Lee Terry (R-Neb.) introduced legislation (HR 2729) — called the Health IT Modernization for Underserved Communities Act — that would allow physician assistants who meet certain requirements to qualify for incentive payments under the meaningful use program, Modern Healthcare reports.
Under the 2009 federal economic stimulus package, health care providers who demonstrate meaningful use of certified electronic health records can qualify for Medicaid and Medicare incentive payments.
According to the American Academy of Physician Assistants, physicians and nurse practitioners can receive incentive payments if Medicaid beneficiaries account for at least 30% of their patient volume (Zigmond, Modern Healthcare, 8/4).
HR 2729 would expand those eligibility requirements so physician assistants could receive the incentive payments if Medicaid beneficiaries account for at least 30% of their patient load (Rodak, Becker’s Hospital Review, 8/4).
In a statement, AAPA President Robert Wooten praised the legislation, saying “this bill extends the promise of improved medical care to the Medicaid patients served by a physician assistant.”
The bill has been referred to the House Energy and Commerce Committee (Modern Healthcare, 8/4).
Source: iHealthBeat
Women are more likely than men to use the Internet to search for health information, according to a new data brief by CDC’s National Center for Health Statistics, HealthDay reports.
The report was based on data from the 2009 National Health Interview Survey, which collected data from 27,731 U.S. adults (Dotinga, HealthDay, 7/21).
Key Findings
The data brief found that women searched online for health data at a higher rate than men across nearly all age groups. The gender gap was largest among adults ages 25 to 34. In that age group, 65.8% of women reported searching for health data on the Internet in the previous 12 months, compared with 44.4% of men.
However, among adults age 65 and older, 24.4% of men had searched online for health data in the previous year, compared with 21.9% of women.
Researchers also found that:
In addition, the data brief noted that people with higher incomes, privately insured individuals and those with more education were more likely to use the Internet to look up health information (Fiore, MedPage Today, 7/25).
Source: iHealthBeat
Earlier this month, CMS released adjustments to its electronic prescribing program that aim to make it easier for health care providers to avoid penalties if they do not meet certain criteria for electronically transmitting Medicare beneficiaries’ prescriptions to pharmacies, Medscape reports.
Background
The Medicare Improvements for Patients and Providers Act established Medicare incentive payments for physicians who e-prescribe with approved software.
The e-prescribing program started paying out incentives in 2009, and Medicare providers who do not e-prescribe are scheduled to face penalties beginning in 2012.
In May, CMS issued a proposed rule that would allow certain physicians to claim exemptions from requirements in the e-prescribing incentive program. The proposed rule also would extend the deadline for physicians to claim such exemptions (iHealthBeat, 5/27). The comment period on the proposed rule ends July 25.
New Proposal Details
Under the newly proposed adjustments to the e-prescribing program, clinicians who fail to earn e-prescribing bonuses in 2011 could avoid penalties in 2013 if they submit 10 or more e-prescriptions during the first half of 2012.
In addition, clinicians could avoid penalties in 2014 if they receive a bonus payment in 2012 or if they report at least 10 e-prescriptions during the first half of 2013.
The new proposal also would apply two of the four exemptions from the 2012 penalty to 2013 and 2014. The two exemptions are:
CMS is accepting comments on the newly proposed adjustments until Aug. 30 (Lowes, Medscape, 7/19).
Source: iHealthBeat
Great! Your office has selected the electronic medical records system, and now, in the fifth article in this series, we need to address the process of getting hardware installed, networks set up, people trained, and the software working for you.
Basic Need
To get a system installed, there will clearly be requirements for hardware (the PCs, servers (if a Client-Server system), networking equipment (the connections both for internal wired and/or wireless networking, and external access to the internet), and installation of the actual software program selected (locally, if a Client-Server, or possibly on each PC if an applet or application is required for a web-based (ASP) product). Indentifying and fulfilling these requirements may be managed in whole or in part by combinations of the vendor, the practice, or consultants.
Environmental
It is extremely important to have qualified people look at the physical placement of servers, understanding the need for physical security as well as environmental requirements for dust, cooling, power supply, back-up power, etc. Security breaches to electronic medical record systems are as often from internal sources as from external (hacking). Being able to lock the server(s), secure PCs with appropriate passwords for log on, etc. are not only good business sense, but specifically addressed in HIPAA and ARRA, with BIG penalties for breaches. Being smart about policies, procedures, and design at the outset will be the most cost-effective solution long term.
Part of the hardware process will need to be assessing any existing technology for its ability to perform appropriately for the new system. Technology that is more than about 18 months old, running on older operating systems, or both should be evaluated for the cost-effectiveness of upgrades versus purchase/lease of new equipment. As mentioned in an earlier article, hardware for a practice really should be of commercial quality, not home office level. The robustness of switches, hubs, routers, wireless devices, etc. is substantially better for business-level, and the cost of down-time, repairs, lost productivity will ultimately greatly exceed the greater expense for the business quality products.
Selection of the specific devices (TabletPCs, notebooks, fixed PCs) should be reflective of the use and role required. Flexibility may suggest that notebooks and tablets be considered even for front office staff (allowing mobility) and nursing staff. The physician staff will also benefit from mobility, particularly if a docking station is used, allowing connection of real keyboards (faster typing) plus recharging of batteries (extending useful battery life and run times). Not having to log in and out when moving from room to room is also a time saver. Wireless access is obviously a requirement for this type of mobility, and proper design of the access points to eliminate dead zones is critical.
Consider placing several PCs in the waiting room for patient check-in, education, and, assuming your vendor has a patient portal, updating of their records.
Be aware of the locations to install printers, and where possible, use fast network printers rather than local printers. The seemingly lower cost of personal printers is in fact much more expensive in the long run: purchasing three or four cheap printers will cost almost as much as a decent network printer and the cost of toner (please don’t use ink!) will certainly be much greater with the small printers than the business class network printer. In other words, the cost per page will be many times greater, and the time it takes to print also many times longer. Critical metrics to look for in a printer are the time to first page out, and pages per minute. Printing of instructions for patients, educational materials (e.g., ACOG brochures), and (hopefully only a relative few) printed prescriptions [electronic prescribing is a requirement for ARRA payment] will be a major source of frustration if it takes 5 minutes to print at the physician’s desk instead of 20 seconds at the central network printer.
Standardize processes
Applicable in offices with more than one physician, the need to standardize as much as possible will make implementation easier and cheaper for everyone. While personalizing some things is easy (favorite medications, most frequently used diagnoses), having completely different lists for each provider just makes things harder, more confusing, and more expensive to implement. Unless the practices have vastly different patient mixes (e.g., one physician practicing general OB/GYN and another only doing uro-gynecology), having common data tables and structure is definitely preferred. Taking all of the existing policies and procedures, protocols, etc. and discussing the desired way to standardize can be done well in advance of the implementation process, and will again save time and money. This concept applies equally to multi-site practices, where standardization will aid in maintaining the product, ease of staff moving between offices, etc.
Training
Despite having seen the product in demonstrations, your knowledge of the best way to use the new EMR purchased will be incomplete. Training is essential for you and your staff to understand the impact on workflows, and how to take advantage of the new tool. Part of this process MUST be changing YOUR workflows to suit the EMR rather than the other way around. In other words: cooking in a microwave oven requires a different technique than cooking on the stove top, and using a pneumatic nail gun to drive a nail does not mean that you whack the nail with the gun like you do with a hammer!
Training methods can include what is called “train-the-trainer”, where only a select few people are trained by the vendor, and the newly trained staff member(s) is/are responsible for training the rest of the staff. The advantage of this can be a reduced cost of training. By only have a few people travel to the training location, or requiring fewer of the vendor staff to travel to your office, expenses can be decreased. The disadvantage is that the vendor’s training staff will usually be more knowledgeable, and better able to answer those edge-case questions. Additionally, the risks of having a fewer number of fully trained personnel include re-training or lost knowledge should that staff leave (illness, relocation, quitting, etc.).
Thus, for larger offices, train-the-trainer is a viable solution, but for small offices, having all the staff trained by the vendor probably makes more sense. Super-users will need to be identified in either scenario, for on-going local support that does not require a call to the vendor is much quicker and more cost effective.
On-line training (web-based) or computer-based training (CBT) may be offered by some vendors, and can also be a cost-effective way of learning the system. This avoids the expense of travel, and, providing the web training is recorded, or CBT courses can be re-run at will, allows refresher classes to be held at the office’s convenience.
Depending again on the size and number of offices and staff to be trained, the sequence of training can vary with regards to staff versus physician training. “Just in Time” training is suggested, meaning the training occurs very shortly before go-live. In cases where the implementation takes many months, if training occurs at the beginning, most of what was learned has been forgotten before it ever gets put to use. It may be wise to consider having the staff go live (and be trained) for some time prior to the physician training and use. Using that method, when the physician first starts using the system, there will be sufficient data already in the EMR to make it more valuable. As you may suspect, it will generally take many months for the existing patient data to be entered in the system (as back-filling is problematic at many levels: expensive, questionable data and accuracy, etc.). One should probably look for at least 9 to 12 months of data entry exceeding the value for most OB/GYNs, except, of course, for the obstetrical patients. (If you see a new or return gynecological patient for her annual exam, unless she returns for a problem, your next encounter with value of the just-entered data is one year later at her next annual exam.)
Scheduling Patients
Recognize that for at least a short while, the office will have a reduced ability to move patients through. Depending on the technical abilities of the staff (typing skills, computer literacy, familiarity with similar programs, etc.), anywhere from a 10% to 25% decreased productivity can be expected. Ask your vendor what their experience is with this, and the anticipated duration of the decrease. For some practices, just a few weeks of this lost productivity is all that would be expected, while for others it may be months.
To avoid increasing frustration levels beyond the breaking point, schedule the patient load accordingly. Particularly during the first few days (or weeks, even), having enough slack in the schedule to not only overcome questions but also work out kinks in workflows will keep the experience positive. Blowing up any good will and enthusiasm for the project for the sake of seeing a few more patients for increased revenue is another penny-wise pound-foolish choice.
Lessons Learned
If you have more than one office and choose to implement the product sequentially, make sure that any issues identified and lessons learned are captured to the benefit of the next office in line. Debriefs with the vendor, trainers, and consultants will help keep the process on track for other offices, and for new modules or functionality introduced by the vendor. Keep track of training issues, and ensure that new employees are brought up to speed incorporating the knowledge learned.
Refresher courses as part of credentialing are recommended; just as your credentialing at the hospital requires CME, so should your practice insist on staff and physicians maintaining their abilities to use the office EMR. ARRA will require capturing significant information on meaningful use and quality metrics as a by-product of use of EMRs.
Next steps
Now that the system is installed, people are trained, and patients are being seen and the visits documented in the EMR, you might think that you are done with this. Wrong!
Just as medicine is not a stagnant field with no new knowledge coming along, neither is this new world of the EMR. There will be updates to the system, new functionalities added, new rules and alerts for the clinical decision support (expert advice) that should be built into the EMR.
All of this requires continued monitoring, continued tweaking, continued adaptation of the office to the dynamics.
Source: ACOG
Work flow analysis and future work flow redesign are often cited as key factors of successful implementations of ambulatory electronic medical records (EMRs) in physician practices. This is the first in a series of blogs to discuss the value of performing workflow analysis before selecting an ambulatory EMR.
It is unfortunate that work flow analysis, if performed at all, is typically not done until an EMR has been selected and the implementation initiated. Although physicians intuitively understand the value of good workflows in the office, how workflow analysis helps the physician choose an EMR is not so obvious.
Workflow analysis can provide the physician practice insights on what to look for in their new EMR product if done early in the selection process. To get the most out of a work flow analysis it is best to start with a clear purpose in mind. Some important reasons for initiating work flow analysis before selecting an EMR are to:
When a work flow analysis is completed the physician practice should expect to see:
A workflow analysis will initially result in written descriptions of the key processes that the physician practice thrives on each day. These written descriptions are then synthesized into a workflow map that may look something like this:
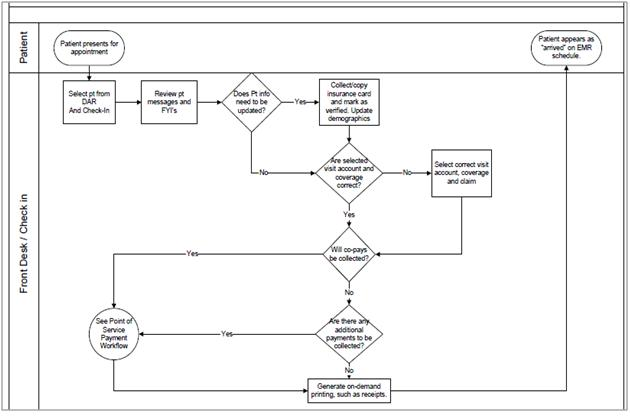
This current workflow map can be used by the practice to design better workflows. Using the current workflow example from above, the draft development of a future workflow map might initially look something like this:
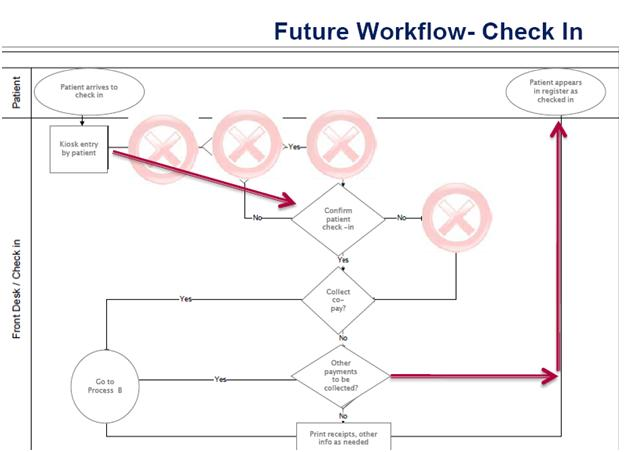
Developing workflow descriptions and critically thinking about desired future workflows will help identify what an EMR needs to be able to do well for the practice. Knowing what the EMR needs to do well will help the practice identify and prioritize needed EMR functionalities.
Source: Digitized Medicine
America’s health system is on the brink of significant transformation. Due to the layered complexity of the health care reform legislation, nearly every participant in the health system will be affected, including providers, patients, payers and government agencies. While providers will have much on their minds in the coming months, from mandates on reimbursement and payment reform to measurement and reporting of care, the most groundbreaking of these changes is the urgency to implement and adopt a system of Electronic Medical Records (EMRs).
As the 2014 deadline for EMR adoption set forth by the American Recovery and Reinvestment Act looms provider organizations face penalties for failing to meet the timeline for demonstrating meaningful use. At the same time the volume of information, available technology options and solutions providers entering market continues to multiply. For leadership teams who may just be starting to mobilize their organizations to implement EMRs, navigating already unfamiliar terrain has now become confusing, complex and fraught with risk. How can providers successfully integrate electronic records and processes and avoid the normal pitfalls that come with inexperience adopting new technologies? By considering the following four values, principals can learn to make the best decisions for adopting EMRs:
While making the switch to EMRs may feel more like a trip through a white-water rapid, these tips provide some insights and principles to focus the organization and help provide navigation aids during the journey. Distilling such a complex process down to a small group of basic principles and fundamentals can help to guide the implementation process, allowing providers to mitigate some of the risks and financial penalties.
Source: Hospital News & More
Recent research about health trends discussed on Twitter is attracting the attention of public health experts, who believe the social media website could provide insight into public perceptions of health-related issues, NPR’s “Shots” reports.
The study authors are slated to present their findings next week at a conference sponsored by the Association for the Advancement of Artificial Intelligence.
Background
Two computer scientists at Johns Hopkins University’s Center for Language and Speech Processing — Mark Dredze, a professor at the university, and Michael Paul, a graduate student — obtained access to about two billion Twitter updates, or tweets, posted between May 2009 and October 2010 (Barclay, “Shots,” NPR, 7/13).
Dredze and Paul developed a filtering software to pull out and categorize health-related tweets. From their original sample, the two researchers filtered out 1.5 million health-related tweets and sorted them into ailment-specific categories (Armstrong Moore, CNET News, 7/11).
Findings
By analyzing the tweets, the researchers identified Twitter discussions about allergies, insomnia, obesity and numerous other conditions. They also found some correlations between influenza rates and flu discussions on Twitter, as well as allergy-related tweets.
In addition, researchers identified tweets that revealed public misconceptions about health issues. For example, they found tweets suggesting that antibiotics could be used as a flu treatment, even though viruses such as influenza are not susceptible to antibiotics.
Health Experts Show Interest
Paul said that the study has received attention among public health experts who are “interested [in] using Twitter to detect misinformation.” He said such experts view Twitter as a “social media tool to mine people’s perceptions of health.”
Dredze said that analyzing tweets could provide information to help guide public health policies. He said, “It could help officials decide what strategies are effective and what are not” (“Shots,” NPR, 7/13).
Study Limitations
Dredze and Paul’s Twitter study has several limitations, according to CNET News. For instance, some people might lie or stretch the truth in their tweets, and some people might refrain from tweeting more personal health issues.
In addition, the study reflects trends only among people who use Twitter, meaning that certain demographic groups — such as seniors — might not be well-represented (CNET News, 7/11).
Source: iHealthBeat
 Is your practice looking for educational videos for your patients? If so, contact us and learn how we can help!
Is your practice looking for educational videos for your patients? If so, contact us and learn how we can help!
The Office of the National Coordinator for Health IT is planning to develop animated videos that explain to consumers the value of health IT, according to an announcement on the Federal Business Opportunities website, Government Health IT reports.
Project Details
ONC plans to hire a vendor to design one or two animated videos, which will be about 10 minutes long or less.
The vendor will be expected to put together a small panel to advise on video style and content, as well as to prepare a draft storyboard for review.
Vendors interested in the project must respond to the announcement by July 26.
Purpose of the Videos
In the announcement, ONC said it wants to increase public demand and support for health IT tools and services to better involve patients in their health care.
ONC also said there is a need to help people identify changes that it is pushing for in the health care system (Mosquera, Government Health IT, 7/12).
Source: iHealthBeat
 Although most hospitals that participated in the American Hospital Association’s 2011 “Most Wired Survey” are moving forward with implementation of clinical care and patient safety technology, they continue to be challenged by federal meaningful use criteria, Hospitals & Health Networks magazine reports.
Although most hospitals that participated in the American Hospital Association’s 2011 “Most Wired Survey” are moving forward with implementation of clinical care and patient safety technology, they continue to be challenged by federal meaningful use criteria, Hospitals & Health Networks magazine reports.
Details of Survey
To determine the Most Wired list, published this month in Hospitals & Health Networks magazine, hospitals were evaluated on four factors:
The survey included additional requirements that corresponded to meaningful use criteria. Under the 2009 economic stimulus package, health care providers who demonstrate meaningful use of certified electronic health record systems can qualify for Medicaid and Medicare incentive payments.
The survey was conducted between Jan. 15 and March 15. This year, 530 hospitals and health systems responded to the survey, representing about 24% of U.S. hospitals, or 1,388 facilities.
Key Survey Results
The list of Most Wired hospitals grew from 99 hospitals in 2010 to 154 organizations this year (Weinstock/Hoppszallern, Hospitals & Health Networks magazine, July 2011).
According to the results, hospitals generally reported strong advances in certain areas of health IT adoption.
Most Wired hospitals reported significant advances in computerized provider order entry.
According to the survey, hospitals generally reported strong advances in certain areas of health IT adoption. Most Wired hospitals reported strong advances in computerized provider order entry.
In addition, the survey found that:
Meaningful Use Still a Challenge
Achieving federal meaningful use criteria continues to be a challenge to all hospitals, including those on the Most Wired list.
For example, 51% of Most Wired hospitals still manually input CMS core measure data into an electronic file.
Meanwhile, only 70% of Most Wired hospitals have the capability to record a problem list of patients’ diagnoses. CMS requires documenting such information for 80% or more of emergency department or admitted patients (Hospitals & Health Networks magazine, July 2011).
Ameican Hospital Association President Weighs In
Commenting on the results, AHA President and CEO Richard Umbdenstock said, “Greater adoption of IT can bring important new tools to our efforts to improve the safety and quality of care in hospitals, and better coordinate care across settings.”
He added, “To promote further use of IT, [AHA is] aggressively working to remove regulatory barriers and provide clarity in areas such as the meaningful use criteria” (AHA News, 7/11).
Source: iHealthBeat
 MGMA Supports ICD-10 Testing With Outside Organizations
July 30, 2013
Report: Many EHR Users Set To Replace Systems Within the Next Year
July 30, 2013
Providers, Vendors Urge Congress To Delay Meaningful Use Stage 2
July 30, 2013
Many Doctors May Find Meeting ‘Meaningful Use’ Requirements a Challenge
June 28, 2013
When it Comes to ICD-10 Physician Documentation: Collaborate and Educate
June 28, 2013
The Slow Crawl Toward Improved EHR Usability and Interoperability
June 28, 2013
Efficient Patient Communication and Engagement
June 13, 2013
ONC Issues Guidance on Stage 2 Transition of Care Requirements
May 31, 2013
Drugmakers Leverage Doctor, Patient Data To Market Their Products
May 31, 2013
Consumer Organizations Defend Meaningful Use Program
May 31, 2013
MGMA Supports ICD-10 Testing With Outside Organizations
July 30, 2013
Report: Many EHR Users Set To Replace Systems Within the Next Year
July 30, 2013
Providers, Vendors Urge Congress To Delay Meaningful Use Stage 2
July 30, 2013
Many Doctors May Find Meeting ‘Meaningful Use’ Requirements a Challenge
June 28, 2013
When it Comes to ICD-10 Physician Documentation: Collaborate and Educate
June 28, 2013
The Slow Crawl Toward Improved EHR Usability and Interoperability
June 28, 2013
Efficient Patient Communication and Engagement
June 13, 2013
ONC Issues Guidance on Stage 2 Transition of Care Requirements
May 31, 2013
Drugmakers Leverage Doctor, Patient Data To Market Their Products
May 31, 2013
Consumer Organizations Defend Meaningful Use Program
May 31, 2013